中国组织工程研究 ›› 2013, Vol. 17 ›› Issue (39): 6887-6895.doi: 10.3969/j.issn.2095-4344.2013.39.005
• 人工假体 artificial prosthesis • 上一篇 下一篇
全膝关节置换后股骨假体周围的骨折
朱兴阳1,苏海涛2,黄永明2
- 1广州中医药大学第二临床医学院,广东省广州市 510405;2广东省中医院骨科,广东省广州市 510006
-
出版日期:2013-09-24发布日期:2013-09-24 -
通讯作者:苏海涛,教授,主任医师,硕士生导师,广东省中医院骨科,广东省广州市 510006 -
作者简介:朱兴阳★,男,1988年生,河南省洛阳市人,汉族,广州中医药大学在读硕士,主要从事髋膝关节疾病的研究。
Periprosthetic femoral fracture after total knee arthroplasty
Zhu Xing-yang1, Su Hai-tao2, Huang Yong-ming2
- 1 Second Clinical Medical College, Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China
2 Department of Orthopedics, Traditional Chinese Medicinal Hospital of Guangdong Province, Guangzhou 510006, Guangdong Province, China
-
Online:2013-09-24Published:2013-09-24 -
Contact:Su Hai-tao, Chief physician, Professor, Master’s supervisor, Department of Orthopedics, Traditional Chinese Medicinal Hospital of Guangdong Province, Guangzhou 510006, Guangdong Province, China suhaitao1234@yahoo.com.cn -
About author:Zhu Xing-yang★, Studying for master’s degree, Second Clinical Medical College, Guangzhou University of Chinese Medicine, Guangzhou 510405, Guangdong Province, China 250040974@qq.com
摘要:
背景:全膝关节置换后股骨假体周围骨折与骨质疏松、骨缺损、假体、患者脆弱以及高并发症发生率等因素有关,其防治较困难。 目的:综合近几年的文献以探讨全膝关节置换后股骨假体周围骨折的危险因素、分型、治疗、康复及预防。 方法:应用计算机分别检索PubMed和Spinger Link数据库相关文献,检索时间分别设定为1990年1月1日至2011年12月31日和1980年至2011年,检索词设定为“periprosthetic fracture, knee”,检索语言设定为英语,共检索到626篇文章。 结果与结论:按纳入和排除标准对文献进行筛选,共纳入40篇文章。结果表明,随着全膝置换在临床中的广泛开展,股骨假体周围骨折的发生率正在逐年增高,因其预后较差,所以要重视其预防,这一骨折的危险因素包括患者自身内在的难以控制的因素和固定技术等外在因素。Rorabeck分型是全膝置换后股骨假体周围骨折最常用的分型方法,但其在临床应用中并不理想;Kim分型将会更有效的指导临床。股骨假体周围骨折的治疗包括非手术治疗、切开复位内固定、逆行髓内钉以及翻修等,合适治疗方案的选择主要取决于骨折的类型、局部骨质量、患者的健康状况等,目前尚缺乏完美的原则来指导选择合适的治疗措施,置换后早期功能锻炼将有益于预防固定过久引起的相关并发症及关节功能的丢失。因此,全膝关节置换后股骨假体周围骨折的治疗要严格把握适应证,在牢固固定的同时,应该尽量鼓励患者早期功能锻炼。
中图分类号:
引用本文
朱兴阳,苏海涛,黄永明. 全膝关节置换后股骨假体周围的骨折[J]. 中国组织工程研究, 2013, 17(39): 6887-6895.
Zhu Xing-yang, Su Hai-tao, Huang Yong-ming. Periprosthetic femoral fracture after total knee arthroplasty[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(39): 6887-6895.
Among the 40 included articles on periprosthetic femoral fracture after total knee arthroplasty[1-40] , 5 articles were about risk factors of periprosthetic femoral fracture[7-11] ,
2 articles were about classification[13-14] , 6 articles were about treatment by plates[15-16, 21, 24-26] , 3 articles were about supplemental bone grafting[17-19] , 4 articles were about intramedullary fixation[4, 27-29] , 3 articles were about extramedullary fixation[31-33] , 5 articles were about revision[34-38] , and 12 articles were about
others[1-6, 12, 20, 22-23, 30, 39-40] .
Risk factor for periprosthetic femoral fracture after total knee arthroplasty
The independent correlation of weight and body mass index with the risk of periprosthetic femoral fracture following total knee arthroplasty has not been clearly demonstrated in the literature. Several other important patient-related and surgical risk factors in this fracture, however, have been identified. Trauma was the major cause of this fracture, and even minor trauma may be sufficient to cause it[2-3] . Documented risk factors of the patient were osteopenia, osteoporosis, female sex, local osteolysis, chronic application of corticosteroids, rheumatoid arthritis and previous revision arthroplasty[1-5] . Female sex, rheumatoid arthritis and chronic steroid application have been associated with an increased risk of periprosthetic femoral fracture because all of them could increase the likelihood of osteoporosis. It was unclear whether steroid application an independent risk factor or an indicator of the severity of rheumatoid arthritis[1] . Merkel et al [3] reported that patients with a revision total knee arthroplasty had a 1.6% incidence (10/637) of periprosthetic femoral fracture compared with 0.6% (26/4 596) for patients with primary total knee arthroplasty. Additionally, patients with neuromuscular disorders, including Parkinson’s disease, epilepsy, cerebellar ataxia, cerebral palsy, myasthenia gravis, poliomyelitis, or undefined neuropathic joints have also been consistently demonstrated to be the higher risk factors for periprosthetic femoral fracture[1-2, 6] .
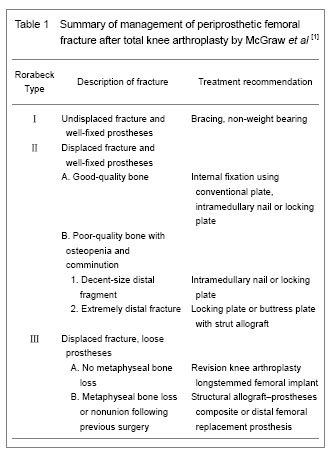
Numerous classification systems have been described for periprosthetic femoral fractures. The comparatively primitive and mature classification of distal femoral fracture was Neer classification, which was based on the displacement and stability and created for fractures in knees without prostheses, so it failed to account for the relationship between the fracture and the implant[1] . The Rorabeck classification is commonly applied[13] , because it takes the displacement of the fracture and prosthesis condition (well fixed or instability) into account. However, it was not a perfect guideline for the selection of appropriate treatment option. A new classification schemes based on the status of the prosthesis, the quality of distal bone stock, and the reducibility of the fracture, proposed by Kim et al [14] , will be better able to guide clinicians. The Orthopaedic Trauma Association classification of femur fractures may additionally be applied in order to design surgical plan.
Diagnosis for periprosthetic femoral fracture after total knee arthroplasty
Most of the periprosthetic femoral fractures following total knee arthroplasty were associated with only slight trauma, so there always, rather than any other fractures, do not have severe edema of the soft tissue. Standard anteroposterior and lateral views are basic for diagnosis. However, before identifying the differential fractural classification, a CT-scan was crucial to define whether any instability of the prosthesis had occurred. In fact, it was not always possible to make a definitive diagnosis of a loose prosthesis especially in a fracture situation since the loosening may be just partial or shielded by the implant. In addition, whether there was a septic loosening before periprosthetic fracture should be identified through assessing patients’ medical history and conventional X-ray. If the patient with a medical history of pain, fever or swelling around the prosthesis before the trauma, it might indicate that there was a previous instability. Therefore, joint aspiration and the analysis for leukocyte count, neutrophil differential, culture, and sometimes frozen section of the synovial fluid, should be recommended to patients with clinical signs of infection.
The goals of treatment, no matter surgical or nonsurgical, were fracture healing, restoration and maintenance of knee range of motion, and pain-free function. A good result was a minimum of 90° of knee motion, fracture shortening for 2 cm, varus/valgus malalignment of 5°, and flexion/extension malalignment of 10°[1] . Sometimes, it was not easy to guarantee whether any loosening of the prosthesis has been occurred preoperatively. Therefore, the orthopedics surgeon should prepare a revision arthroplasty when an osteosynthesis was initially planned.
Nonoperative treatment for periprosthetic femoral fracture after total knee arthroplasty: Conservative methods, which included skeletal traction, plaster of paris and non-weight bearing of the knee for several weeks, were generally recommended for undisplaced fractures with a stable fixed prosthesis (Rorabeck Ⅰ or Kim IA). The advantages of nonoperative management were that it could eliminate surgical risks such as bleeding, infection and anesthetic complications. Nevertheless, immobilization in non-operative treatment always causes loss of motion and reduces walking capacity. Several studies have reported satisfactory results of fracture consolidation following nonoperative treatment. However, most of authors were not willing to reveal any data concerning knee function or systemic complications after the nonoperative treatment. Culp et al [6] reported the result in thirty patients treated nonoperatively. Fifteen patients (50%) had increased pain or decreased ambulatory status following nonoperative care, whereas this was only 13% of patients treated operatively. Harlow and Hoffman reviewed 142 periprosthetic femoral fractures treated conservatively and found that 29% of these fractures eventually required reoperation[12] .
Open reduction internal fixation with conventional plates for periprosthetic femoral fracture after total knee arthroplasty: The aim of open reduction and internal fixation was to provide anatomical reconstruction and early rehabilitation for the patients. Conventional plates mainly include buttress plates, angle blade plates, and dynamic condylar screws which are initially internal fixation devices. However, it is difficult to achieve rigid internal fixation especially for those with significant osteopenia, osteoporosis or comminuted bones. A literature suggested that the lateral condylar buttress plate, which is not a fixed-angle device, had lead to secondary collapse up to 42% of the comminuted distal femur fractures[15]. The blade plate and the dynamic condylar screws which can offer fixed angular stability distally make some progresses. Yet, it is a pity that they cannot be utilized in total knee arthroplasty with intramedullary stems and are not well suited to minimally invasive techniques.
| [1]Su ET, DeWal H, Di Cesare PE. Periprosthetic femoral fractures above total knee replacements. J Am Acad Orthop Surg. 2004;12(1):12-20. [2]McGraw P, Kumar A. Periprosthetic fractures of the femur after total knee arthroplasty. J Orthop Traumatol. 2010; 11(3):135-141. [3]Merkel KD, Johnson EW. Supracondylar fracture of the femur after total knee arthroplasty. J Bone Joint Surg. 1986;68(1):29-43. [4]Chettiar K, Jackson MP, Brewin J, et al. Supracondylar periprosthetic femoral fractures following total knee arthroplasty: treatment with a retrograde intramedullary nail. Int Orthop. 2009;33(4):981-985. [5]Bong MR, Egol KA, Koval KJ, et al. Comparison of the LISS and a retrograde-inserted supracondylar intramedullary nail for fixation of a periprosthetic distal femur fracture proximal to a total knee arthroplasty. J Arthroplasty. 2002;17(7): 876-881. [6]Culp RW, Schmidt RG, Hanks G, et al. Supracondylar fracture of the femur following prosthetic knee arthroplasty. Clin Orthop Relat Res. 1987;(222):212-222. [7]Completo A, Fonseca F, Relvas C, et al. Improved stability with intramedullary stem after anterior femoral notching in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2012;20(3):487-494. [8]Lesh M, Schneider D, Deol G, et al. The consequences of anterior femoral notching in total knee arthroplasty: a biomechanical study. J Bone Joint Surg. 2000;82(8): 1096-1010. [9]Shawen SB, Belmont PJ Jr, Klemme WR, et al. Osteoporosis and anterior femoral notching in periprosthetic supracondylar femoral fractures: a biomechanical analysis. J Bone Joint Surg. 2003;85(1):115-121. [10]Zalzal P, Backstein D, Gross A, et al. Notching of the anterior femoral cortex during total knee arthroplasty characteristics-that increase local stresses. J Arthroplasty. 2006;21(5):737-743. [11]Ritter MA, Thong AE, Keating M, et al. The effect of femoral notching during total knee arthroplasty on the prevalence of postoperative femoral fractures and on clinical outcome. J Bone Joint Surg. 2005;87(11):2411-2414. [12]Dennis DA. Periprosthetic fractures following total knee arthroplasty. Instr Course Lect. 2001;50:379-389. [13]Rorabeck CH, Taylor JW. Classification of periprosthetic fractures complicating total knee arthroplasty. Orthop Clin North. 1999;30(2):209-214. [14]Kim KI, Egol KA, Hozack WJ, et al. Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res. 2006; 446:167-175. [15]Davison BL. Varus collapse of comminuted distal femur fractures after open reduction and internal fixation with a lateral condylar buttress plate. Am J Orthop (Belle Mead NJ). 2003;32(1):27-30. [16]Healy WL, Siliski JM, Incavo SJ. Operative treatment of distal femoral fractures proximal to total knee replacements. J Bone Joint Surg. 1993;75(1):27-34. [17]Virolainen P, Mokka J, Seppänen M, et al. Up to 10 years follow up of the use of 71 cortical allografts (strut-grafts) for the treatment of periprosthetic fractures. Scand J Surg. 2010;99(4):240-243. [18]Wang JW, Wang CJ. Supracondylar fractures of the femur above total knee arthroplasties with cortical allograft struts. J Arthroplasty. 2002;17(3):365-372. [19]Kumar A, Chambers I, Maistrelli G, et al. Management of periprosthethic fracture above total knee arthroplasty using intramedullary fibular allograft and plate fixation. J Arthroplasty. 2008;23(4):554-558. [20]Althausen PL, Lee MA, Finkemeier CG, et al. Operative stabilization of supracondylar femur fractures above total knee arthroplasty: a comparison of four treatment methods. J Arthroplasty. 2003;18(7):834-839. [21]Raab GE, Davis CM. Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty. 2005;20(8):984-989. [22]Ehlinger M, Adam P, Abane L, et al. Treatment of periprosthetic femoral fractures of the knee. Knee Surg Sports Traumatol Arthrosc. 2011;19(9):1473-1478. [23]Parvizi J, Jain N, Schmidt AH. Periprosthetic knee fractures. J Orthop Trauma. 2008;22(9):663-671. [24]Kregor PJ, Hughes JL, Cole PA. Fixation of distal femoral fractures above total knee arthroplasty utilizing the Less Invasive Stabilization System (LISS). Injury. 2001;32 Suppl 3:64-75. [25]Ricci WM, Loftus T, Cox C, et al. Locked plates combined with minimally invasive insertion technique for the treatment of periprosthetic supracondylar femur fractures above a total knee arthroplasty. J Orthop Trauma. 2006;20(3):190-196. [26]Erhardt JB, Grob K, Roderer G, et al. Treatment of periprosthetic femur fractures with the non-contact bridging plate: a new angular stable implant. Arch Orthop Trauma Surg. 2008;128(4):409-416. [27]Ritter MA, Keating EM, Faris PM, et al. Rush rod fixation of supracondylar fractures above total knee arthroplasties. J Arthroplasty. 1995;10(2):213-216. [28]Gliatis J, Megas P, Panagiotopoulos E, et al. Midterm results of treatment with a retrograde nail for supracondylar periprosthetic fractures of the femur following total knee arthroplasty. J Orthop Trauma. 2005;19(3):164-170. [29]Han HS, Oh KW, Kang SB. Retrograde intramedullary nailing for periprosthetic supracondylar fractures of the femur after total knee arthroplasty. Clin Orthop Surg. 2009;1(4):201-206. [30]Herrera DA, Kregor PJ, Cole PA, et al. Treatment of acute distal femur fractures above a total knee arthroplasty—systematic review of 415 cases (1981–2006). Acta Orthop. 2008;79(1):22-27. [31]Simon RG, Brinker MR. Use of Ilizarov external fixation for a periprosthetic supracondylar femur fracture. J Arthroplasty. 1999;14(1):118-121. [32]Hurson C, Synnott K, McCormack D. Above-knee Ilizarov external fixation for early periprosthetic supracondylar femoral fracture-a case report. Knee. 2005;12(2):145-147. [33]Pleva L, Sír M, Madeja R. Our experiences with the treatment of periprosthetic fractures of femur. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2004; 148(1): 75-79. [34]Srinivasan K, Macdonald DA, Tzioupis CC, et al. Role of long stem revision knee prosthesis in periprosthetic and complex distal femoral fractures: a review of eight patients. Injury. 2005;36(9):1094-1102. [35]Berend KR, Lombardi AV Jr. Distal femoral replacement in nontumor cases with severe bone loss and instability. Clin Orthop Relat Res. 2009;467(2):485-492. [36]Pour AE, Parvizi J, Slenker N, et al. Rotating hinged total knee replacement: use with caution. J Bone Joint Surg. 2007;89(8):1735-1741. [37]Kassab M, Zalzal P, Azores GMS, et al. Management of periprosthetic femoral fractures after total knee arthroplasty using a distal femoral allograft. J Arthroplasty. 2004;19(3): 361-368. [38]Backstein D, Safir O, Gross A. Management of bone loss: structural grafts in revision total knee arthroplasty. Clin Orthop. 2006;446:104-112. [39]Ehlinger M, Adam P, Moser T, et al. Type C periprosthetic fracture treated with locking plate fixation with a mean follow up of 2.5 years. Orthop Traumatol Surg Res. 2010; 96(1):42-47. [40]Prieto-Alhambra D, Javaid MK, Judge A, et al. Bisphosphonate use and risk of post-operative fracture among patients undergoing a total knee replacement for knee osteoarthritis: a propensity score analysis. Osteoporos Int. 2011;22(5):1555-1571. |
| [1] | 王金军, 邓增发, 刘 康, 何智勇, 余新平, 梁建基, 李 晨, 郭洲洋. 全膝关节置换静脉滴注氨甲环酸联合含氨甲环酸鸡尾酒局部应用的止血效果及安全性[J]. 中国组织工程研究, 2021, 25(9): 1356-1361. |
| [2] | 张 冲, 刘志昂, 姚帅辉, 高军胜, 姜 岩, 张 陆. 局部应用氨甲环酸减少老年股骨颈骨折全髋关节置换后引流的安全和有效性[J]. 中国组织工程研究, 2021, 25(9): 1381-1386. |
| [3] | 吕 振, 白金柱. 基于McKenzie技术的腰椎运动链训练应用于腰椎间孔镜术后分期康复的前瞻性研究[J]. 中国组织工程研究, 2021, 25(9): 1398-1403. |
| [4] | 陈心敏, 李文标, 熊凯凯, 熊晓燕, 郑利钦, 李木生, 郑永泽, 林梓凌. 钉道强化股骨近端防旋髓内钉治疗老年A3.3型股骨转子间骨折:最佳骨水泥量有限元分析[J]. 中国组织工程研究, 2021, 25(9): 1404-1409. |
| [5] | 杜秀鹏, 杨朝晖. 65岁以下嵌插型股骨颈骨折初始畸形程度对颈缩短的影响[J]. 中国组织工程研究, 2021, 25(9): 1410-1416. |
| [6] | 陈俊名, 岳 辰, 何沛霖, 张俊涛, 孙墨渊, 刘又文. 髋关节置换与股骨近端防旋髓内钉内固定修复高龄股骨转子间骨折效果的Meta分析[J]. 中国组织工程研究, 2021, 25(9): 1452-1457. |
| [7] | 陈进平, 李 奎, 陈 骞, 郭浩然, 张映波, 蔚 芃. 开放性脊柱手术应用氨甲环酸的疗效及安全性的Meta分析[J]. 中国组织工程研究, 2021, 25(9): 1458-1464. |
| [8] | 姬志祥, 蓝常贡. 尿酸盐转运蛋白在痛风中的多态性和治疗相关性[J]. 中国组织工程研究, 2021, 25(8): 1290-1298. |
| [9] | 李中峰, 陈明海, 凡一诺, 魏秋实, 何 伟, 陈镇秋. 右归饮治疗激素性股骨头坏死作用机制的网络药理学分析[J]. 中国组织工程研究, 2021, 25(8): 1256-1263. |
| [10] | 万 然, 史 旭, 刘京松, 王岩松. 间充质干细胞分泌组治疗脊髓损伤的研究进展[J]. 中国组织工程研究, 2021, 25(7): 1088-1095. |
| [11] | 焦 慧, 张一宁, 宋雨晴, 林 宇, 王秀丽. 乳腺癌类器官研究进展及临床应用前景[J]. 中国组织工程研究, 2021, 25(7): 1122-1128. |
| [12] | 蔡群斌, 邹 霞, 胡剑涛, 陈心敏, 郑利钦, 黄培镇, 林梓凌, 姜自伟. 有限元法分析尖顶距与股骨近端防旋髓内钉固定股骨转子间骨折稳定性的关系[J]. 中国组织工程研究, 2021, 25(6): 831-836. |
| [13] | 赵中溢, 李勇阵, 陈 峰, 季爱玉. 同期双侧全膝关节置换和单髁置换治疗创伤性关节炎的比较[J]. 中国组织工程研究, 2021, 25(6): 854-859. |
| [14] | 袁 俊, 杨家福. 局部氨甲环酸浸润在非骨水泥全膝关节置换过程中止血效果的评价[J]. 中国组织工程研究, 2021, 25(6): 873-877. |
| [15] | 刘立华, 孙 伟, 王云亭, 高福强, 程立明, 李子荣, 王江宁. 头颈部开窗减压治疗L1型激素性股骨头坏死:单中心前瞻性临床研究[J]. 中国组织工程研究, 2021, 25(6): 906-911. |
Data sources
The Rorabeck classification is commonly applied, but it is not a perfect guideline for selection of appropriate treatment option. Kim classification, based on the status of the prosthesis, the quality of distal bone stock and the reducibility of the fracture, will be better able to guide clinicians. As for the treatment, nonoperative treatment and external fixation are mainly adapted to those who accompanied with significant comorbidities or those who are too weakness to undergo the internal fixation. Retrograde intramedullary locking nailing is widely used, but it is unsuitable for very distal or severe comminuted fractures. What’s more, it has to be proven that the distal femoral prosthesis is open before planning this implant osteosynthesis. Revision arthroplasty is mainly used for a comminuted or extremely distal fracture where secure fixation cannot be achieved. Recent studies have manifested great advantages of less invasive stabilization system plate which have already added to the list of viable fixation options. In brief, the optimized choice of treatment is up to a number of factors that include the adequacy of bone stock, the degree of displacement, condition of the implant and the medical fitness of the patient. Rehabilitation is the important step, so it must be continued. Early exercise is beneficial for functional recovery and can prevent the postoperative complications of immobilization. Due to the devastating consequence and complicated treatment of periprosthetic femoral fracture, attentions should not only be paid to the treatment, but also to the prophylaxis. Patient factors such as osteoporosis play a significant role in increasing the risk of these fractures.
1 全膝关节置换后股骨假体周围骨折的治疗方法很多,但均不理想。 2 文章详细剖析了全膝关节置换后股骨假体周围骨折的危险因素、分类、治疗及康复,将对临床该类骨折的防治起到参考作用。 3 结果证实,全膝关节置换后股骨假体周围骨折合适治疗方案的制定必须综合考虑骨折的类型、宿主骨质量、骨折端移位情况、假体松动与否、患者的身体状况等多重因素,内固定后早期功能锻炼是减少关节功能丧失的重要康复措施。
文章设计思路: 全膝关节置换后股骨假体周围骨折一般指关节线以上15 cm以内的骨折或是股骨假体柄末端5 cm以下的骨折,股骨假体周围骨折是全膝关节置换后假体周围骨折中最常见的类型。据报道全膝置换后股骨假体周围骨折在初次全膝关节置换后的发生率为0.3%-2.5%,在翻修术后的发生率为1.6%-38.0%。此类骨折可以在术后立即发生,亦可以在骨折后数十年后发生。随着全膝置换患者寿命的延长、活动量的增大以及全膝关节翻修术数量的增加,全膝关节置换后股骨假体周围骨折的发生率近年来也在不断升高,但由于患者骨质量差、高龄、多并存病、股骨远端有限的内固定空间、假体潜在不稳定等诸多因素的制约。文章将对全膝关节置换后股骨假体周围骨折的危险因素、分型、治疗、康复及预防方面进行详细探讨,以便为该类骨折防治提供参考。
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||